
Effective patient care hinges on clear, concise communication – and that starts with well-organized notes. A robust nurse notes template is an invaluable tool, streamlining workflows, reducing errors, and ultimately, enhancing the patient experience. This guide will delve into the essential components of a successful nurse notes template, providing you with the knowledge to create and utilize a system that supports optimal patient care. Nurse Notes Template is more than just a document; it's a strategic asset for any nurse. It's a foundation for accurate record-keeping, facilitating seamless transitions between shifts, and ensuring continuity of care. Let's explore how to build a template that truly works for you.
Understanding the Importance of Nurse Notes
The modern healthcare landscape demands efficiency and accuracy. Nurses are often juggling multiple tasks simultaneously – monitoring vital signs, administering medications, assessing patient conditions, and coordinating care with physicians. A disorganized or incomplete record can lead to miscommunication, delayed interventions, and potentially, adverse patient outcomes. A well-structured nurse notes template minimizes these risks by providing a readily accessible and easily digestible record of patient information. It's a critical component of patient safety and a cornerstone of a professional nurse's practice. The ability to quickly and accurately capture essential details empowers nurses to make informed decisions and respond effectively to patient needs. Furthermore, standardized templates contribute to inter-professional communication, fostering a collaborative environment.
Core Components of a Nurse Notes Template
A truly effective nurse notes template should include several key elements. It's not simply a list of observations; it's a structured approach to documenting patient information. Here's a breakdown of the essential components:

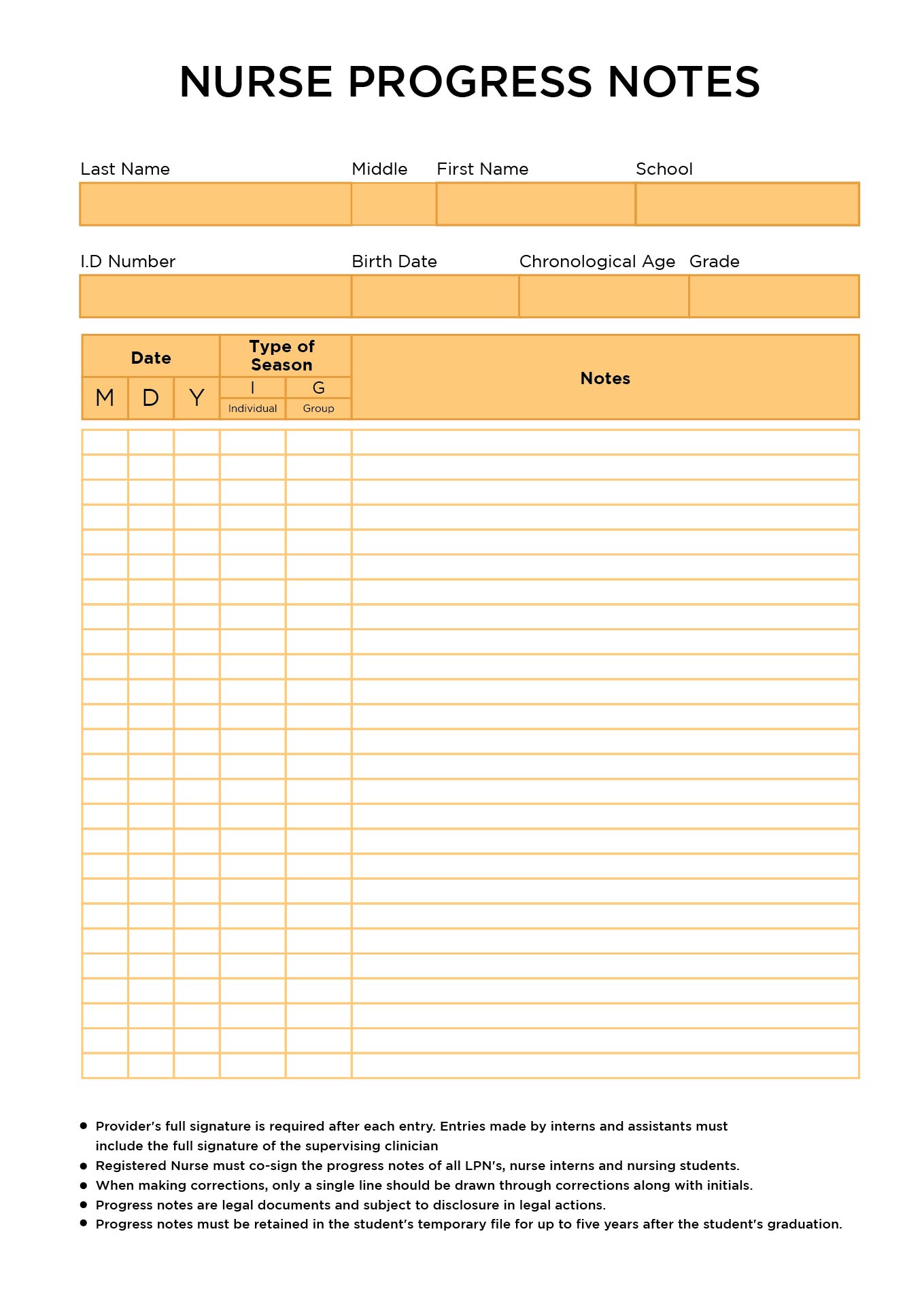
1. Patient Identification
The first step is always accurately identifying the patient. This includes the patient's full name, date of birth, and any relevant medical record number. Double-check this information to ensure accuracy – a single typo can have significant consequences. A clear and consistent format is crucial for efficient data entry. Consider using a standardized format for patient identification, such as:
.png)
- Patient Name: _
- Date of Birth: _
- Medical Record Number: _
- Signature: _
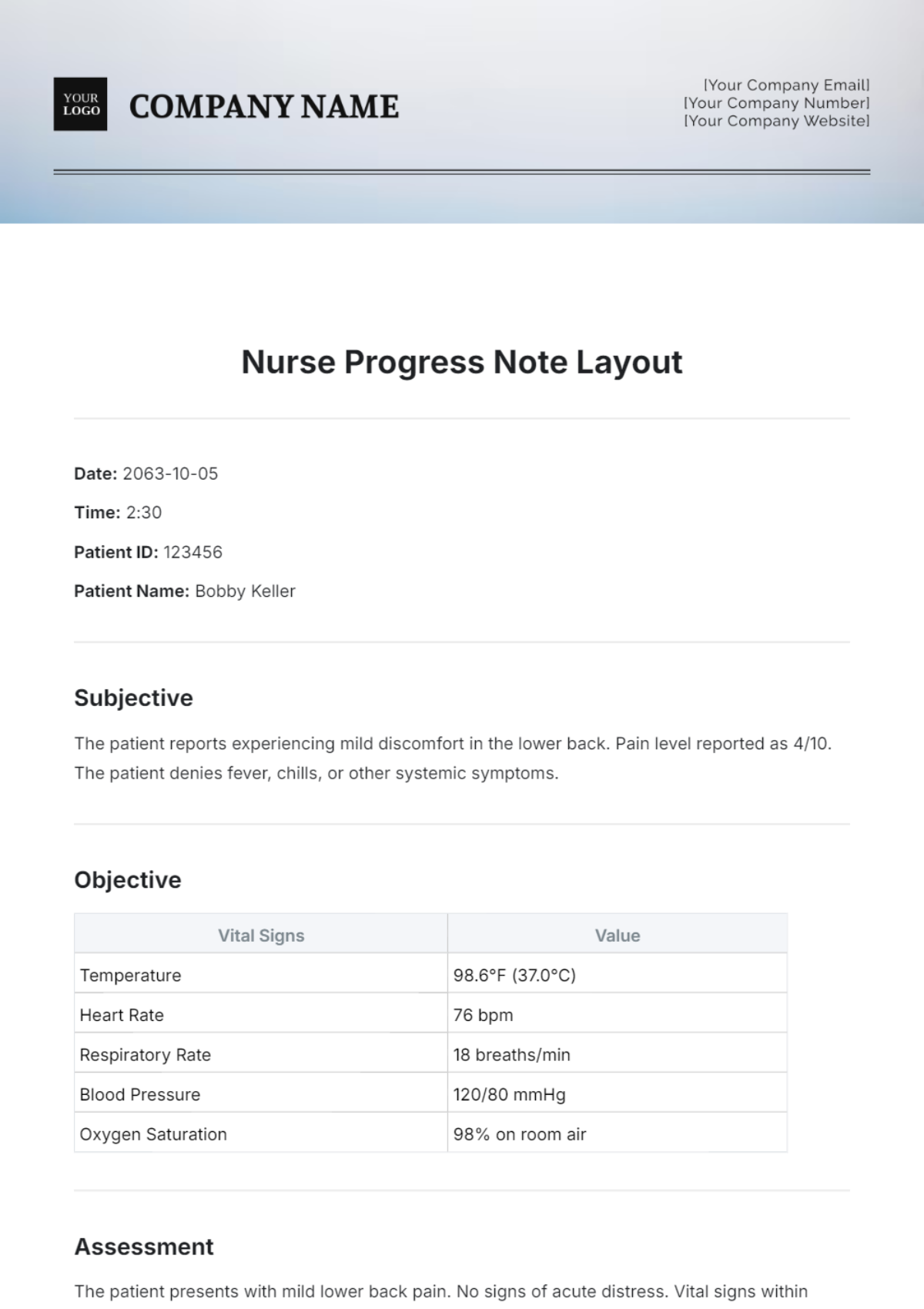
2. Date and Time of Visit
Precisely recording the date and time of the visit is vital for tracking trends and ensuring continuity of care. The time should be recorded in 24-hour format (e.g., 08:00 AM). This allows for easy chronological ordering of events.

- Date: _
- Time: _
3. Reason for Visit
Clearly state the reason for the patient's visit. This helps to understand the context of the patient's condition and guides subsequent care plans. Be specific and concise.
- Reason for Visit: _
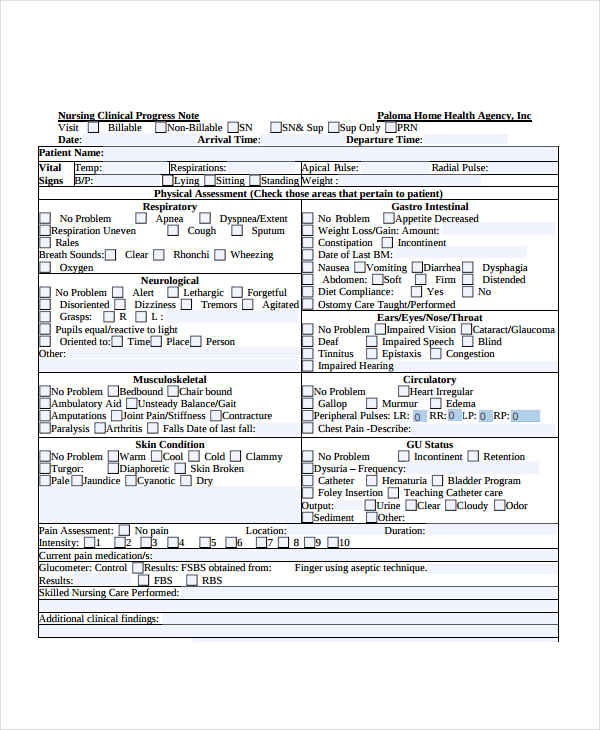
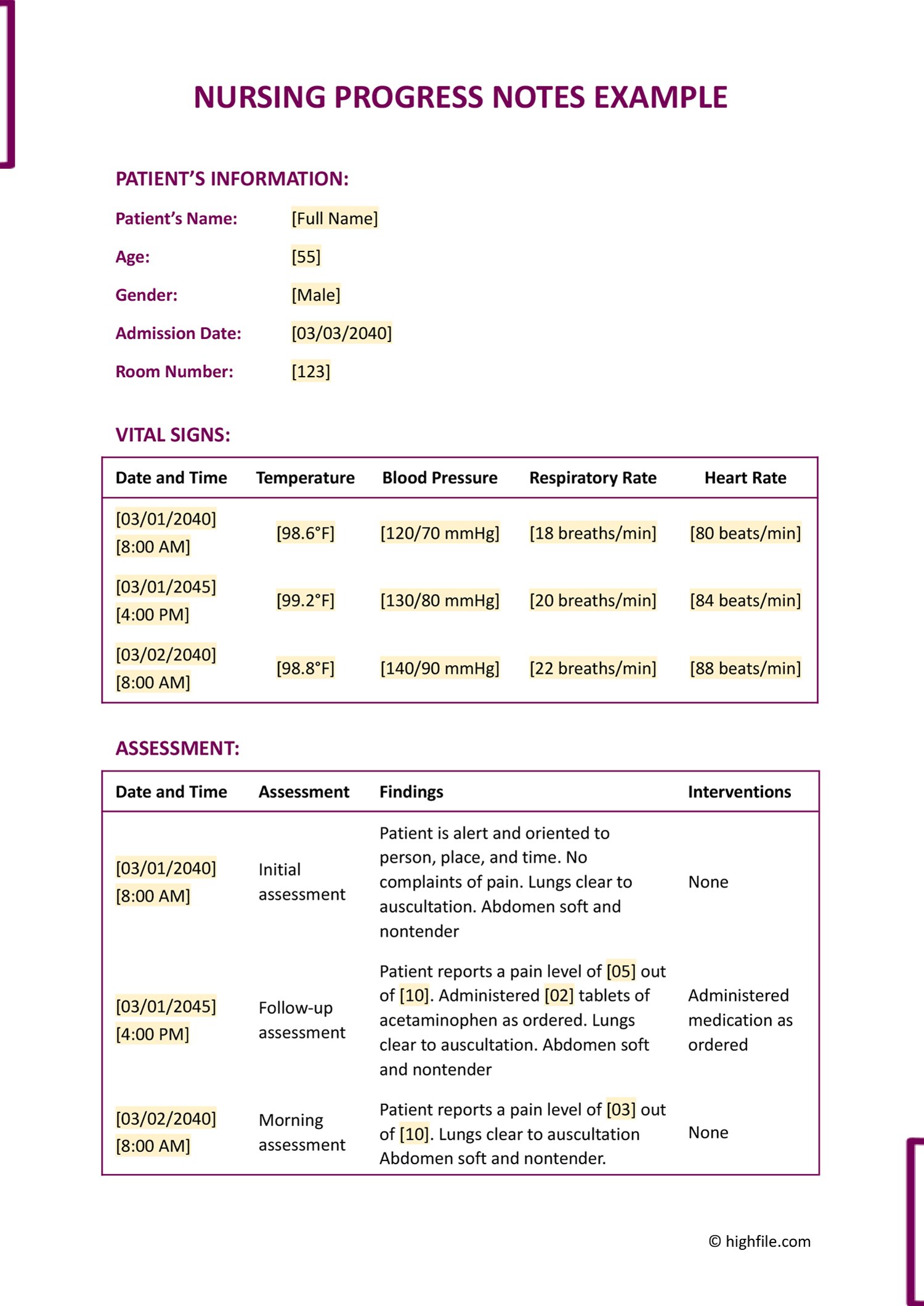
4. Vital Signs
Accurate vital sign recording is paramount. Record temperature, pulse, respiration rate, blood pressure, and oxygen saturation. Always include units of measurement (e.g., °C, bpm, mmHg). Document any abnormal readings immediately.
- Temperature: _ °C
- Pulse: _ bpm
- Respiration Rate: _ breaths/min
- Blood Pressure: _ mmHg
- Oxygen Saturation: _ %
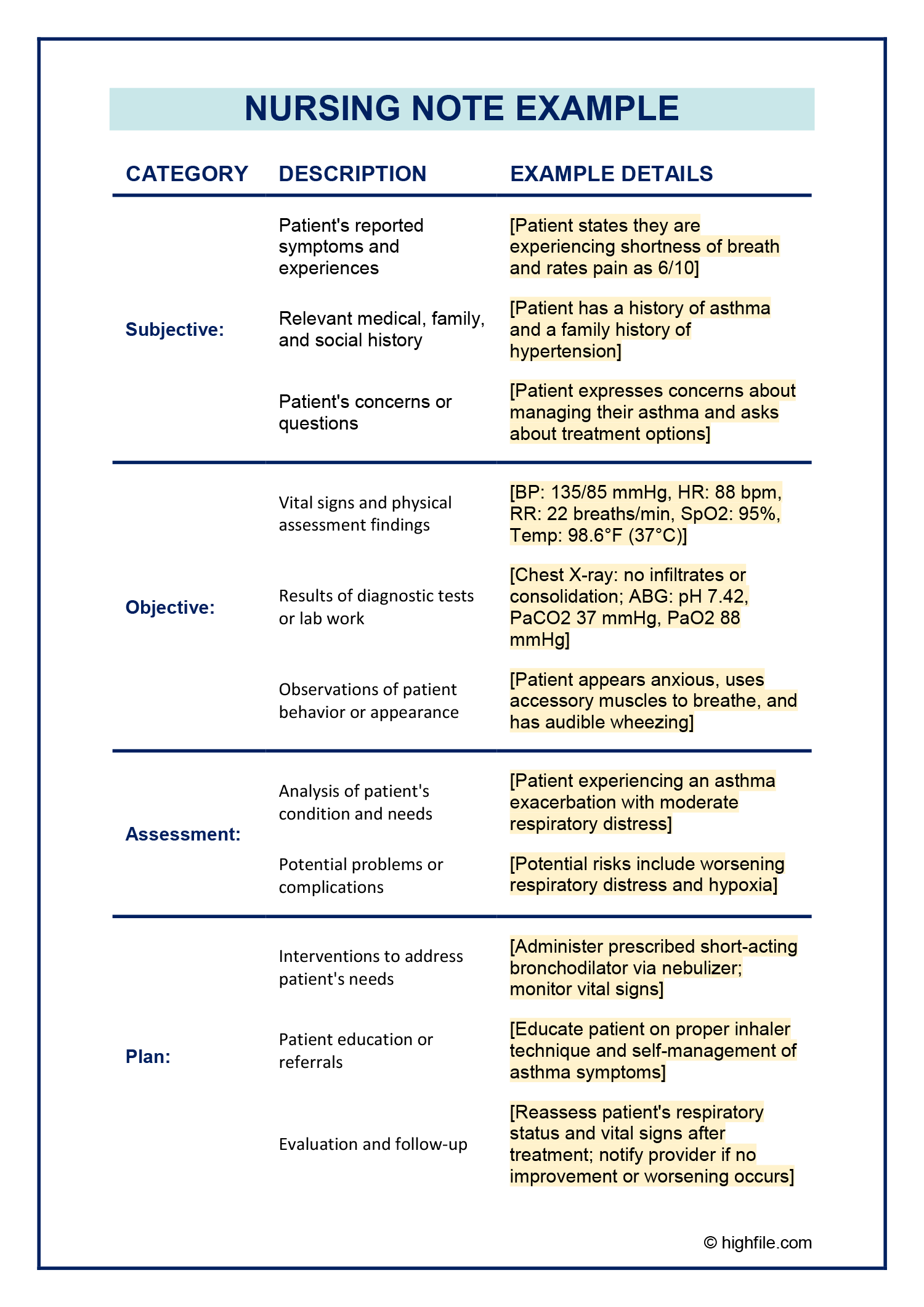
5. Assessment Findings
This section summarizes the nurse's assessment of the patient's condition. It should include a concise description of the patient's overall appearance, mental status, and any significant findings. Use descriptive language to paint a clear picture of the patient's state.

- Overall Appearance: _ (e.g., Alert, confused, pale)
- Mental Status: _ (e.g., Oriented, confused, lethargic)
- Neurological: _ (e.g., Motor strength, sensation, reflexes)
- Respiratory: _ (e.g., Respiratory rate, effort, breath sounds)
- Cardiovascular: _ (e.g., Heart rate, rhythm, murmurs)
- Gastrointestinal: _ (e.g., Bowel sounds, presence of nausea)
- Skin: _ (e.g., Dry, moist, rashes)
6. Medications and Allergies
Document all medications the patient is taking, including the dosage, route of administration, and frequency. Also, record any allergies the patient has, including the type of reaction. This is crucial for preventing adverse drug interactions.

- Medication: _
- Dosage:
- Route:
- Frequency:
- Allergy: (e.g., Penicillin, hives)
- Allergies: _ (e.g., Penicillin, hives)
7. Nursing Interventions
Describe the nursing interventions performed during the visit. Be specific about the actions taken and the rationale behind them.
- Intervention 1: _ (e.g., Administered medication, repositioned patient)
- Intervention 2: _ (e.g., Provided comfort measures, monitored vital signs)
- Intervention 3: _ (e.g., Educated patient on medication administration)
8. Plan of Care
This section outlines the nursing plan for the patient. It should include specific goals, interventions, and anticipated outcomes. It's a roadmap for the next shift.
- Goal: _
- Interventions: _
- Expected Outcome: _
The Importance of Standardization and Iteration
While a standardized nurse notes template provides a solid foundation, it's important to remember that it's a living document. Regularly review and update the template to ensure it remains relevant and effective. Solicit feedback from colleagues and supervisors to identify areas for improvement. Consider incorporating a system for tracking and analyzing notes to identify trends and potential issues. Nurse Notes Template should be a tool for continuous improvement, not a static set of rules.
Conclusion: Leveraging a Robust Nurse Notes Template for Optimal Patient Care
A well-structured and consistently utilized nurse notes template is an indispensable asset for any healthcare professional. By prioritizing accurate documentation, clear communication, and a proactive approach to patient care, nurses can significantly improve patient outcomes and enhance the overall quality of care. Investing time in developing and maintaining a robust template is an investment in patient safety and professional excellence. Ultimately, a thoughtfully designed template empowers nurses to provide the best possible care, contributing to a healthier and happier community. Nurse Notes Template is a critical component of a nurse's professional toolkit.
Additional Resources
- [Link to a reputable nursing note template resource]
- [Link to an article on effective communication in healthcare]
- [Link to a guide on patient safety protocols]
0 Response to "Nurse Notes Template"
Posting Komentar